Hypothesis Testing for Difference Between Groups
Introduction
Healthcare systems often rely on MHA FPX 5017 Assessment 2 Hypothesis Testing Between Groups analysis to make informed decisions regarding resource allocation and implementation of improvement strategies. In this analysis, we investigated the performance of two rural healthcare clinics based on the total number of visits per month. The objective is to determine if there is a significant difference between the clinics and provide recommendations for improvement based on the findings.
Hypothesis Formulation for Group Difference Analysis
We began by formulating hypotheses to test the difference between the two clinics:
Null Hypothesis (H0): There is no significant difference in the total number of visits per month between Clinic 1 and Clinic 2.
Alternative Hypothesis (H1): There is a significant difference in the total monthly visits between Clinic 1 and 2.
Formulating a hypothesis can benefit from phrasing the problem as a question. This approach aids in clarifying what will be tested and which variables will be utilized (Kros & Rosenthal, 2016). In this scenario, we might ask: Are Clinics 1 and 2 equally productive, or does one exhibit a higher average number of monthly visits than the other?
Data Analysis
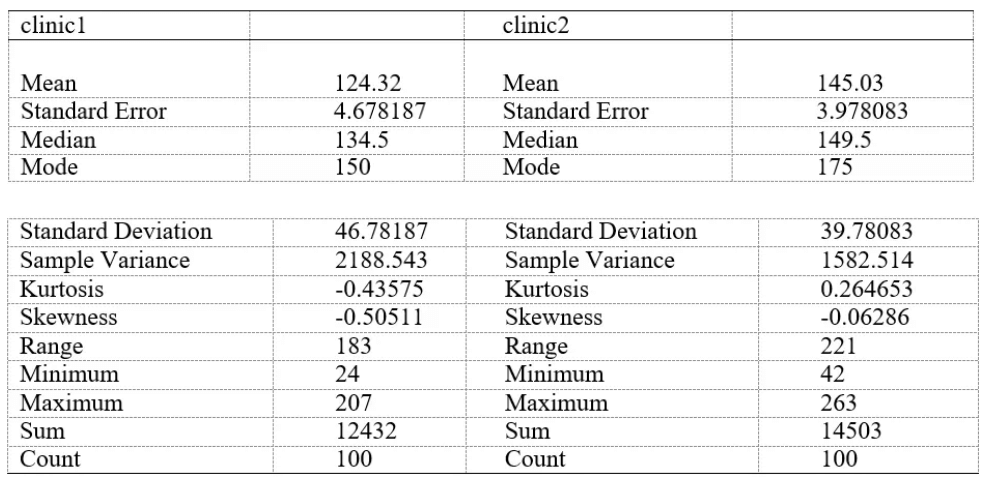
Based on the results provided, several observations can be made. Firstly, Clinic 1 demonstrates a mean productivity of 124.32 visits per day, whereas Clinic 2 exhibits an average of 145.03 per day based on 100 observations for each clinic. Additionally, there appears to be a notable difference in the variance between the two clinics, with Clinic 2’s average daily visits closer to the mean compared to Clinic 1, as noted by (Trinh et al., 2021).
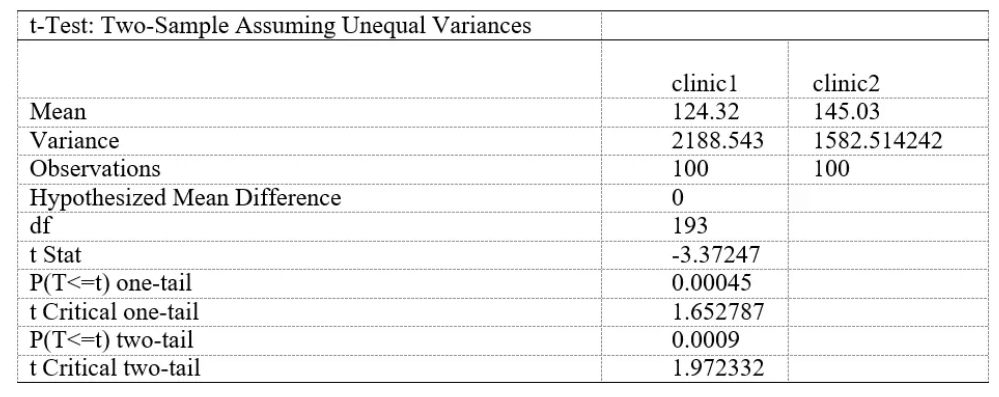
Moreover, the T-statistic of 3.372+ indicates the distance from zero of the standard error, with higher values (preferably above 2) implying greater confidence in the coefficient. Combined with the p-value, it aids in determining whether to accept or reject the null hypothesis (H0). In this instance, the two-tailed p-value is calculated to be 0.000895937, considerably lower than the alpha level of 0.02. Typically, a p-value below the alpha threshold suggests a statistically significant difference between the two samples, with lower p-values indicating greater confidence in this significance.
Consequently, based on the presented data, substantial evidence suggests that the productivity disparity between Clinic 1 and Clinic 2 is statistically significant. As a result, the null hypothesis (H0) can be rejected in favor of the alternative hypothesis (Ha).
Conclusion
The examination of the sample data from both clinics suggests that Clinic 2 demonstrates higher productivity, defined by the average number of visits per day, based on a 100-day sampling period. The t-test results provide confidence in extrapolating this finding to the broader population of Clinic 2 visit history. However, it is essential to acknowledge limitations in relying solely on this performance indicator to determine the practical significance of the statistical findings in guiding investment decisions between the two clinics.
MHA FPX 5017 Assessment 2 Hypothesis Testing Between Groups
Limitations in our analysis include whether days with low visit numbers were full-day schedules or half-days and the overall capacity of the respective clinics. Another factor is how many providers are in each clinic, which can contribute to how many patients are seen daily. Therefore, making informed investment decisions requires a comprehensive assessment considering various factors beyond visit numbers.
Multiple factors contribute to assessing the overall performance of a healthcare practice, as outlined by the Medical Group Management Association. These factors include RVUs (Relative Value Units) per physician, claims denial rate, number of days cash on hand, employee turnover, patient satisfaction scores, payor mix, no-show rate, and third next available (Opelka, 2005). More than relying on one performance indicator would be required to make an informed decision about purchasing a new clinic. Therefore, this analysis recommends delving deeper into these additional financial and performance metrics for both clinics before concluding. While the initial results may appear promising, obtaining further information is crucial to ensure a well-informed and financially sound decision.
References
Kros, J. F., & Rosenthal, D. A. (2015). Statistics for health care management and administration: Working with Excel (public health/epidemiology and biostatistics) (3rd ed.). Jossey-Bass.
Opelka, F. G. (2005). Office financial evaluation and management. Clinics in Colon and Rectal Surgery, 18(04), 271–278. https://doi.org/10.1055/s-2005-922851
Trinh, P., Hoover, D. R., & Sonnenberg, F. A. (2021). Time-of-day changes in physician clinical decision making: A retrospective study. PLOS ONE, 16(9), e0257500. https://doi.org/10.1371/journal.pone.0257500